

Updates in C Diff: Rapid Review of the 2018 IDSA Guidelines
Q: Should I send stool for C. difficile testing for all my inpatients with diarrhea? Should I retest within 7 days if the first test is negative, and should I send a test for cure?
The Bottom Line: NO!
- Don’t test your patient for C. diff if they had < 3 unformed stools in the past day.
- Don’t test patients who received laxatives within the past 48 hours.
- Don’t retest within 7 days.
- Don’t test for cure.
Hospitalized patients could have multiple reasons for loose stools. C. diff commonly colonizes the colon and a positive test may not mean that C. diff. is the cause of diarrhea. By following these simple rules, up to 30% of low-risk patients would not be tested¹ which translates into decreased hospital costs and prevents unnecessary treatment.
Context: Diarrhea is common in the hospitalized patient.¹ Physicians frequently reflexively test for C. diff when diarrhea is present; however, the majority of cases of diarrhea are due to medications, underlying illnesses and enteral feeding. Antibiotic-associated diarrhea is common, but only 20% of cases are caused by C. diff toxin.² Many patients are unnecessarily tested for C. diff when they do not have any diarrhea or signs and symptoms of C. diff disease.
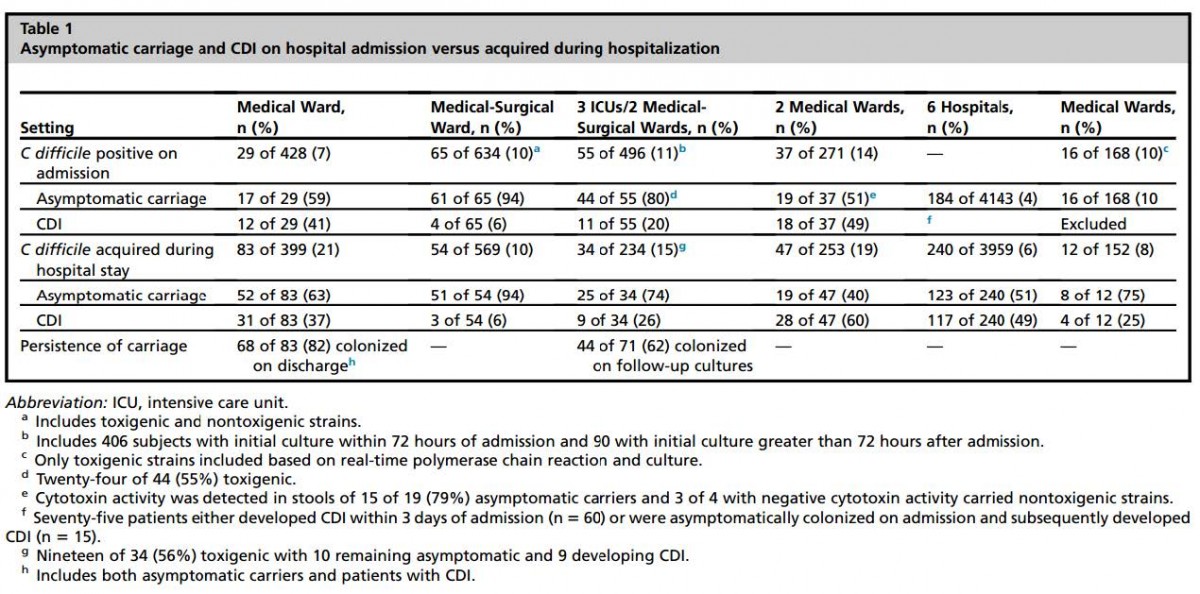
The Data: Asymptomatic colonization of patients with C. diff is increasing.³ Treatment of colonized patients results in unnecessary antibiotic administration, rising hospitalization costs and poor quality metrics for the hospital. Prevalence of C. diff colonization of patients on hospital admission ranges between 7-18%. Acquisition during hospitalization is also rising and is estimated to be between 6-21%. Some studies estimate that 50% of patients hospitalized longer than one month develop colonization, and most will be asymptomatic.³ (Table 1)
C. diff PCR is a highly sensitive test (90%).4 In fact, it is so sensitive that it may be positive and detect the C. diff toxin gene even when the gene is not actively producing toxin. This results in many patients who have a positive test and do not have C. diff infection; i.e. a low positive predictive value for C diff infection (50-70%).5 Positive predictive value increases when the C. diff test is used among patients with a higher prevalence for C. diff infection, such as patients with 3 or more liquid stools per day who have not received laxatives within the past 48 hours.
There is little value of repeat C. diff testing; only 1.7% of people with a negative test have a positive test within 7 days and repeat testing can increase the number of false positive results.6
Repeat stool testing for test of cure is NOT recommended.7 Up to 50% of patients have positive C diff PCR for as long as six weeks after the completion of therapy.8 Therefore, signs and symptoms rather than repeat testing should be used to assess whether a patient has responded to therapy for C. diff.
Conclusion: High rates of C. diff colonization of the colon exist in hospitalized patients. Over-testing among patients without signs and symptoms of C. diff infection can lead to false positive results. Test only those patients who are symptomatic with ≥3 loose stools per day and who have not been exposed to laxatives within 48 hours. Retesting within 7 days of a negative test is usually not clinically indicated. Do not test for cure.
- J Gen Intern Med. 1997 Jan; 12(1): 57–62 PMID: 9034947
- Clin Infect Dis. 2012 Oct;55(7):982-9 PMID: 22700831
- Infect Dis Clin North Am. 2015 Mar;29(1):13-28 PMID: 25595843
- Clin Infect Dis. 2011 Oct;53(7):e81-90. PMID: 21890762
- Infect Control Hosp Epidemiol. 2015 Feb;36(2):217-21 PMID: 25633006
- J Clin Microbiol. 2008 Nov;46(11):3795-7. PMID: 18784320
- Infect Control Hosp Epidemiol. 2010 May;31(5):431-55. PMID: 20307191
- Am J Med. 1989 Jan;86(1):15-9. PMID: 2910090
-The DOM High Value Care Committee

Can you clarify the risk of spreading C.Diff from colonized patients to other patients if loose stool is not tested in the patient that received laxatives within 48 hours. I would like to see the evidence to support the practice of not testing patients receiving laxatives. The inherent risk of exposure to C.Diff spores by not testing does not seem to be an effective solution to preventing spread of C.Diff in the hospital. It would seem not testing (>3 diarrhea stools) r/t laxatives allows for the potential for spread and lack of proper decontamination.
Pingback: Weekly Progress Notes March 30, 2016 | The Hub
Comments are closed.